
Having Children
November 26, 2021
HDYO has more information about HD available for young people, parents and professionals on our site:
www.hdyo.org

Updated in 2023 by Education and Research Committees
Knowing that you are at risk of Huntington's disease may have an impact on how you plan to start a family. The decision to start a family, and how you may go about doing so, is a very personal choice between you and your partner. This section looks at some of the options available with regards to having children.
The genetic risk to children
The risk of passing on HD may be a concern when at-risk people are thinking of having children. A lot depends on whether or not the person wanting children knows their own genetic status. There is a 50% chance that an at-risk person inherited HD from their affected parent. Therefore, if an at-risk person has not had genetic testing, each of their children theoretically has a 25% (1 in 4) chance of inheriting the condition.
Some people decide to test before they have children to find out if they have inherited HD, and therefore, knowing if there is an increased risk of passing on the disease to their pregnancy.
- If an at-risk person has genetic testing and receives a negative test result (they will not develop HD), they are not at risk to have a child affected with HD.
- If an at-risk person has genetic testing and receives a positive test result (they will develop HD at some point in life), there is a 50% (1 in 2) chance of passing HD on in each pregnancy.
Making decisions
Family planning is a time of very personal and complex decision-making when living at-risk of HD, and each individual may approach this time from a different perspective.
Some people take the stance that they will never have children because they do not want to have a child at risk or have that child grow up in a family affected by Huntington's disease. Other people go ahead and have children at risk, because there is a chance the child will not have the expanded gene, or they feel there will be good treatments or even a cure available by the time the child grows up.
Others want to have children, but want to reduce the risk of them inheriting Huntington's disease. Technology and science has made this more of a possibility, and there are a number of options available that may provide a child free of the risk of Huntington's disease.
HDYO has put together a list of the options available to people looking to have children.
Having children: The options
- Conceiving Naturally
- Prenatal Testing
- Exclusion Testing
- Preimplantation Genetic Testing (PGT)
- Egg/Sperm/Embryo donation
- Adoption/Fostering
Conceiving Naturally Without Genetic Testing to the Embryo
Although a lot of this section focuses on the options of having children without an increased risk of HD, it is important to highlight that having children at risk is an option too. Some people elect to grow their family with no medical interventions. These individuals may feel that with advances in HD research, there will be good treatments, or even a cure, by the time the child grows up. Others choose this route because there is a chance the child will not inherit the expanded gene and will never develop HD.

Some people may want to have a child without the risk, but feel they have no available options. For example, fertility treatments may not be available in all countries, individuals may lack the financial support to pursue costly treatments, or families may have religious beliefs that preclude many of the risk-reducing strategies.
The decision around how and when to grow your family can be very personal and complex. Having children at risk is something that may cause debate among family members, and people may not agree with the decisions others make on this issue. That decision, like any on this topic, should be respected.
Prenatal Testing
Prenatal testing involves testing a pregnancy for HD during the first or second trimester (when this can be done varies locally)
Prenatal testing is usually done when a couple is certain that they'll terminate the pregnancy if the genetic test is positive. That decision has to be made beforehand. This is because testing a pregnancy, but not going ahead with a termination after a positive test result, would take away the child's right to choose whether to have the genetic test, later in life.
Who can have prenatal testing?
Prenatal testing can be performed when a parent already knows their HD status, meaning they have tested and received a positive result, OR when a parent is at risk and wishes to remain untested. The latter is known as Exclusion testing (non-disclosing testing).
Exclusion Testing
Exclusion testing involves testing a pregnancy in the first or second trimester (when this can be done varies locally)to see if it has the tracking marker for HD. It is essentially the same process as prenatal testing but with a couple of key differences.
Who can have exclusion testing?
Exclusion testing is specifically for people who want to remain untested but also want a child who isn’t at risk for HD.
Exclusion: The process
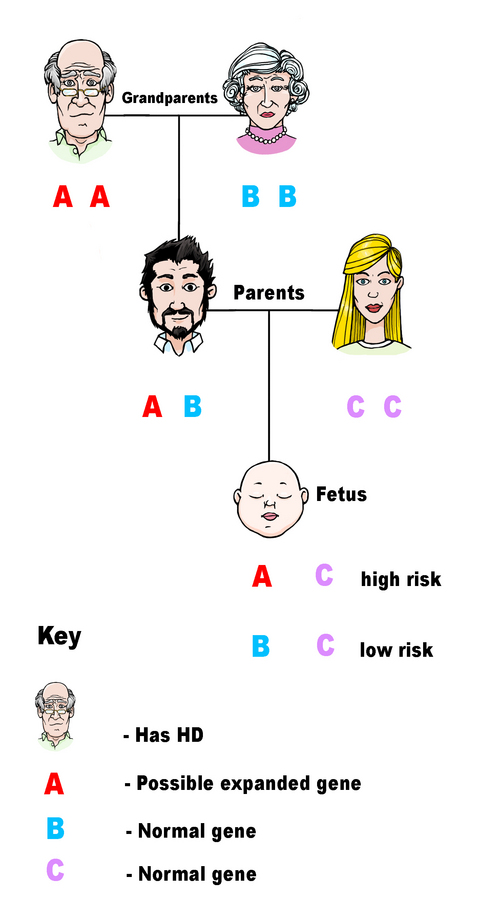
Exclusion testing collects three samples: one from the pregnancy, a second from the person at risk of HD and a third from the at-risk person’s affected parent. The affected family member’s sample is key to the whole process, as the extra sample is used to link and trace which genes the pregnancy has inherited.
Exclusion testing focuses on the section of DNA that contains the HD gene, and attempts to determine whether or not the pregnancy inherited that section from the affected grandparent. If the pregnancy has not inherited it, then the risk of disease is very low. However, if the pregnancy has inherited it, then there is a 50% risk that the child will develop HD.
The major problem with exclusion testing is that it doesn't reveal whether the pregnancy has inherited the normal gene or the expanded gene - only whether or not it has inherited the stretch of DNA from the affected grandparent or not. This is to protect the person at risk who does not want to learn their own status during this process. So, exclusion testing cannot be as precise as prenatal testing. This is why some people may choose to either be tested themselves or use a process such as PGT, where embryos are screened for HD before implantation.
Preimplantation Genetic Testing (PGT)

PGT is a procedure in which an individual’s eggs and an individual’s sperm are retrieved, and an embryo is fertilized in a laboratory. These embryos are then tested to see if they are affected with HD. Only an embryo that does not have a risk of HD will be transferred into an individual. The hope is that a pregnancy will follow. The success rate varies by a range of factors, including the number of eggs retrieved and fertilized, the number of embryos that survive the test, and the number of embryos with the expanded HD gene. If the whole process is successful, then that child will be born free of the risk of HD. Any remaining unaffected embryos can be stored for later use if desired.
The PGT process can be a lengthy and emotional journey, with individuals having to undergo various tests and procedures which can be strenuous at times. There may also be a lot of travelling involved to undergo treatment, and some may have to take time off work. In addition, unsuccessful attempts may be difficult to cope with emotionally. However, for those that come out of the process with a successful pregnancy, PGT can be a very worthwhile option.
Who is PGT available to?
PGT can be pursued by those who have tested positive for HD, or those at risk. For someone who is untested, the process can be done without that person having to learn their HD status - using techniques similar to exclusion testing, described above. Again, this requires getting blood samples from the affected parent of the person going through PGT - although this is not always necessary. This is usually called exclusion PGT, or non-disclosure PGT.
PGT may not be covered by health insurance, and may be costly depending on where you live. Some countries have PGT attempts included in their national health services, which will cover the costs of the procedure. It may also not be available everywhere, with some countries not having the infrastructure to do the procedure or some even banning PGT for religious, ethical and moral reasons. Speak with a genetic counselor or other genetics specialist to see whether PGT is available in your country.
Egg/Sperm/Embryo Donation
This method uses an egg donor or sperm donor in place of the affected parent - meaning a child will not be at increased risk of inheriting HD. Embryo donation is also available in some places. The process is done through a qualified donor clinic. Pregnancy success rates vary between clinics.

At some point, you may decide to tell your child that the affected person is not their biological parent and why this is the case. Depending on which country you have had your treatment, information about their genetic parent may be available via a donor bank. Some donors are what they call 'non-anonymous', meaning that their information is available should the child want to contact them later in life. Other donors are anonymous and contact cannot be sought in the future. Whether the donor is anonymous or not can depend on the rules of the country the procedure is being conducted in. Procedures vary in different areas, so be sure to check and discuss what is available in your area. Again, this is something that you will need to consider if you go down this route, and support may also be available through organisations such as the Donor Conception Network.
Who can use the egg/sperm/embryo donation option?
The egg or sperm donation option can be used by anyone (at risk or tested). The egg/sperm donors themselves are screened for numerous genetic conditions, to minimize the risk of passing on other genetic conditions. The risk of the child developing HD and other screened genetic disorders is quite low (although not zero percent). However, it is important to remember that not all genetic conditions can be screened. Egg/sperm/embryo donation may be an expensive option if funded privately but is often cheaper than PGT depending on the clinic.
Adoption/Fostering
Adoption is when a couple or a family takes in a child who needs a family to look after them. Adoption is generally considered an option for those wishing to have a child at decreased risk of developing HD.
However, couples at risk of HD may find it difficult to adopt because of the disease in their family. At the beginning of the adoption process, an assessment is done on every individual/couple/family wanting to adopt a child, and each situation is carefully considered for the child's sake. The adoption agency wants to make sure that the child has a stable home to go to, and the chance that one of the parents could have HD may be seen as risky. However, each case is assessed individually, so do not rule out adoption as an option. If it is of interest to you and your partner, it is certainly worth looking into and discussing with your local adoption agency, or another health care professional in your area.

You may find that an adoption agency does introductory sessions that you can attend without making any firm commitments to adopt. They will be able to tell you more about both adoption and the potential impact of HD on your prospects of adopting. You may also be able to meet parents who have adopted in the past, who can tell you about their experiences and answer any questions you might have.
Depending on the country you live in, adoption can be a long process, as it takes time to go through the preliminary assessments, workshops and formalities before matching can begin. The time taken to match will depend on your requirements and theirs, how many children you are looking to adopt, what ages you would consider, etc.
Fostering is also an option, even if you have been turned down for adoption on the basis of the future risk of HD. You may still be eligible for fostering because it is a more short term option caring for children for weeks or months at a time. Again, discuss this option with your local adoption agency, or another health care professional in your area to find out more.
On a final note, if you’re from the LGBTQIA+ community, many of these options may be available to you. We highly recommend making an appointment with a genetic counselor near you to talk over your options. If you would like to discuss your circumstances with us, you may contact us.
Support
Support and advice for having children can come from various places. Your National Huntington's disease organization can often provide both support and advice with regards to decisions about having children. HDYO can also help by discussing things in this section that you possibly did not understand fully or would like to learn more about. We can also put you in touch with local support in your area.
If you want specialist information and would like to discuss your options with a professional, then your local HD clinic or clinical genetics department can help you with that. Walking through your options with a genetic counselor or therapist can help you see your own thoughts more clearly and provide strategies to help you cope in difficult situations which may arise on your journey to start a family. You may want to do this individually, or as a couple/family.
Having children is a big decision, one that can be made even more challenging by the impact of HD. As you have seen, there are many options available, and selecting the right one for you and your family can involve a lot of thinking and discussions with those around you. Friends and family play a vital role in providing support, but you may find that they do not always understand what you are going through, no matter how well you explain how you are feeling. They may not agree with the decisions that you and/or your partner make. Ultimately, the important thing is making a decision that is the best for you and your family. You may find that you change your mind over time, and there's no harm in having a Plan B if things don't work out quite as you first intended.


